





1. There is a skin cancer epidemic
Melanoma kills twice as many Britons as cancer of the cervix, well over 2000 a year and rising.1 Fear of melanoma is driving increased public concern and, as ever, the message is ‘if you are worried, see your GP’. So point number one is that every family doctor must have skin lesion recognition skills that are fit for purpose – this means training in dermoscopy. This is not an optional add-on, it’s a core skill like diagnosing headache, cough or childhood fevers.
2. Efficient skin lesion triage is cost effective
Early diagnosis of melanoma saves lives and dermoscopy is THE tool for early diagnosis2, so it could save the NHS millions if adequately deployed. The new drugs for advanced melanoma are promising, but fantastically expensive: one patient with metastatic melanoma may cost $250,000 a year.3
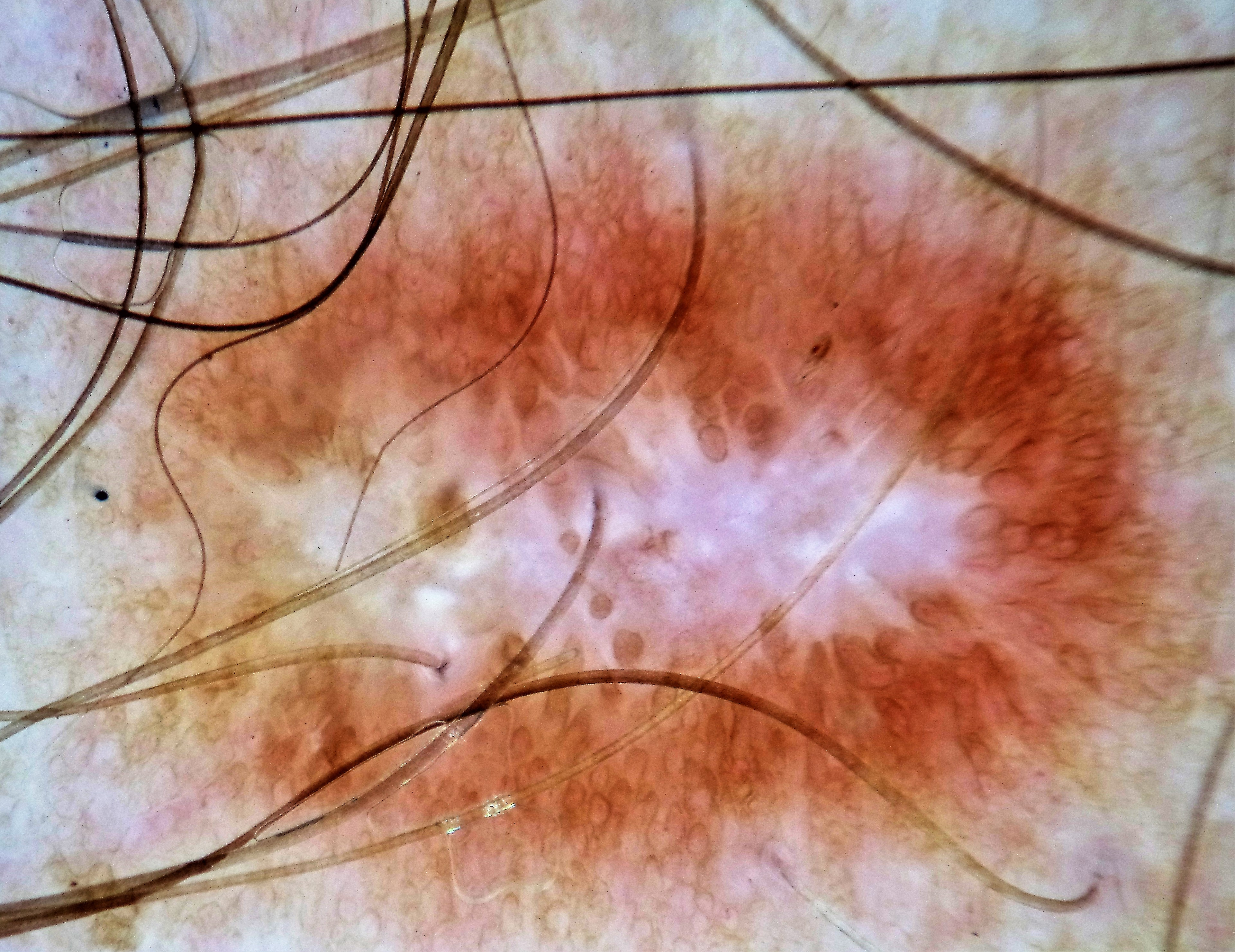
Dermatofibroma with central white area and peripheral brown circles
3. Dermoscopes aren’t cheap, but quickly pay for themselves
Dermoscopy is supported by bags of global peer-reviewed evidence. Dermoscopes are not cheap (a good one can cost £800-£1200) but the cost should be borne by the overall health economy and will quickly pay for itself by reduced referral rates if obviously benign lesions are screened out.
4. Dermoscopy is the key to efficient lesion triage
Haemangiomas, solar lentigos and seborrhoeic keratoses are particularly easy to diagnose, and yes I still see these lesions in every clinic sent up on urgent cancer pathways. This doesn’t just waste the scarce dermatologist resource (delaying the care of your patients with horrible acne, eczema and psoriasis) but terrifies people, as the word ‘cancer’ is on the clinic paperwork they receive.
5. Dermoscopy skills can be learned quickly
As with learning to play the guitar, expertise takes years to acquire, but much can be achieved in a few weeks with appropriate tuition. A well-designed controlled trial4 showed that just one day’s training made a big difference to GPs’ diagnostic skills.
6. There are many excellent dermoscopy videos on YouTube
I can’t think of a better way to get started or at least decide if you are interested. Start with those by the International Dermoscopy Society (IDS). These short, clear videos cover all aspects of dermoscopy for beginners and improvers and can be watched again and again for free. Other web resources include Ian McColl’s longer instructional videos (Google ‘dermoscopy made simple’), French dermatologist Eric Ehrsam’s great blog at dermoscopic.blogspot.com, or you could join the IDS (free) and take part in their online case discussions (also see point 7).
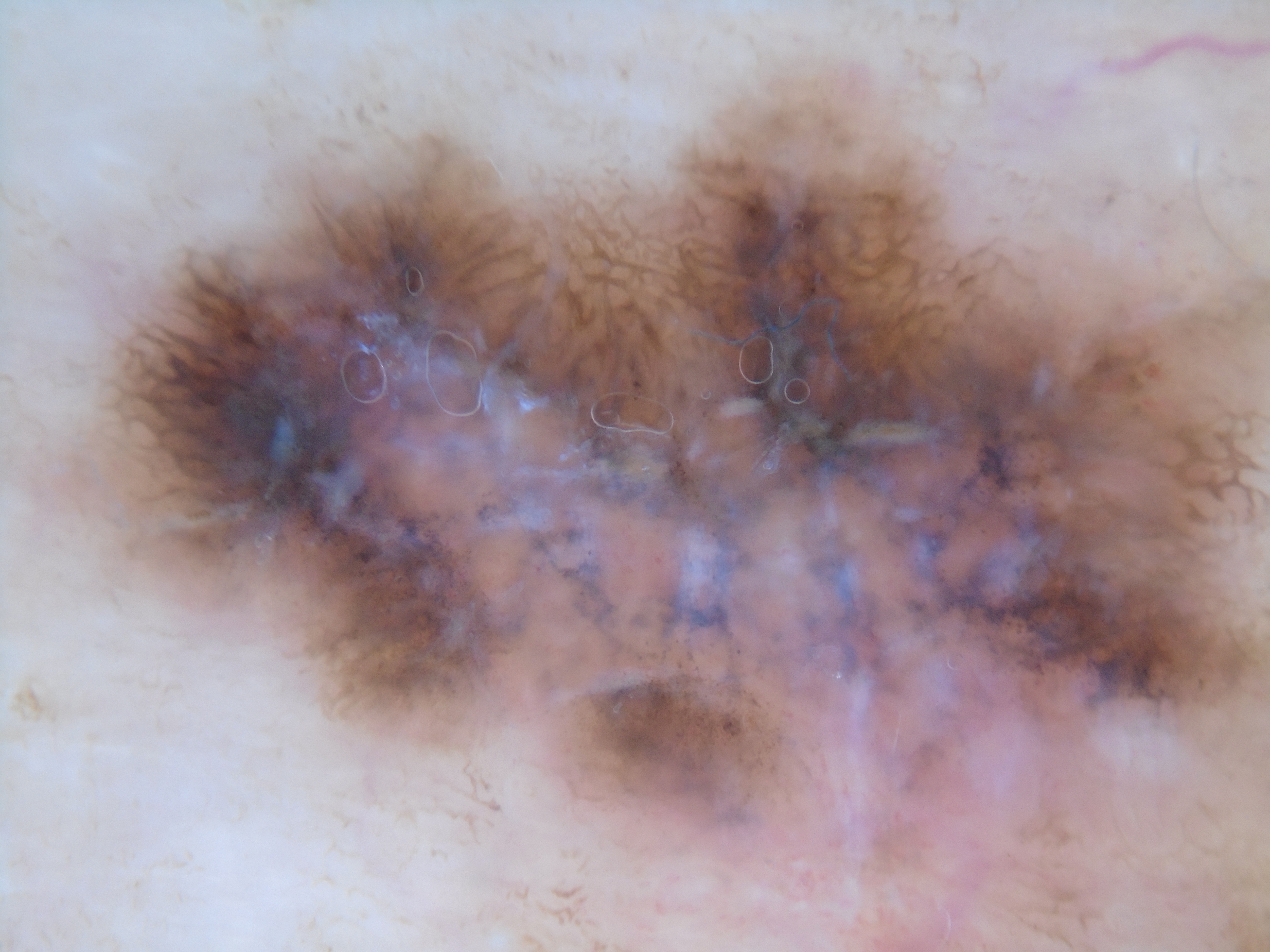
Melanoma with chaos, shiny white streaks and multiple colours
7. Dermoscopy (or dermatoscopy) is also on Facebook
The IDS has a Facebook page with 15,000 global doctors signed up, run by the excellent Bengu Nisa Akay from Ankara, Turkey. You have to ask to join the group but it’s open to all doctors and free. New images and discussions are posted daily. If you are interested in improving your skin lesion recognition skills, consider joining this friendly international group and, as with the YouTube videos, make notes and screen shots for perfectly legitimate CME credits for your appraisal portfolio.
8. There are plenty of courses to go on
The Primary Care Dermatology Society continues at the forefront of UK dermoscopy education with ‘Dermoscopy for Beginners’ courses held around the country. The PCDS also offers advanced day courses with top British dermoscopy teacher Jonathan Bowling, who also runs courses in Oxford, and occasionally brings top international experts over to put on dermoscopy masterclasses. More advanced courses leading to internationally recognised dermoscopy diplomas are held in Graz, Austria, and Queensland, Australia. GPs who are interested in a new career option in skin lesion recognition (private or NHS) might consider investing in these international diploma courses.
9. Dermoscopy is fun
In these grim days, anything that boosts your job satisfaction is to be received with thanks. There is great fulfilment to be found in reassuring an anxious patient that their oddly shaped pigmented lesion is not the cancer they fear but a seborrhoiec keratosis or ink spot lentigo.
In the near future, I believe it will come to be seen as unprofessional, even negligent, to evaluate suspicious skin lesions without dermoscopy, so hopefully people will start to adopt this affordable and effective technique.
Dr Stephen Hayes worked as a GP from 1985 to 2012, a GPSI from 2000 to 2012, and is currently Associate Specialist in Dermatology at University Hospital Southampton. He has taught with the PCDS since 2002 and also teaches independently for reward. He is a UK board member of the International Dermoscopy Society and blogs about dermoscopy at www.dermoscopy.wordpress.com.









