




Case
A 72-year-old male presents to his GP with low back pain, as well as cramping and pain in the buttocks, posterior thighs and calves that severely restricts his mobility. He finds the pain is relieved several minutes after the cessation of walking, by sitting or lying down. The man has visited his GP over the past 10 years with these symptoms and managed them with prescribed physiotherapy, activity modification and analgesia. Despite this, the symptoms are getting worse, and he has come to the GP because he is now struggling to walk to his local shops, although stooping forward offers some relief.
On examination, the symptoms are found to be worse on extension of the spine and improved on flexion. Otherwise, a full neurological examination is normal. The GP suspects lumbar spinal stenosis that may require surgical management, and refers him to a spinal surgeon.
The problem
Spinal stenosis is a narrowing within the spinal canal or the channels through which the spinal nerves exit the spinal canal. This causes compression of the spinal nerves.
The most common cause of spinal stenosis is age-related arthritic degeneration of the spinal canal. Spinal stenosis can also sometimes be caused by a slipped disc, infection, fractures, or even a tumour. In a small number of cases it could be caused by congenital narrowing of the spinal canal.
Features
The signs and symptoms of spinal stenosis are usually of gradual onset from the age of 60 onwards and, if they progress, will do so slowly over a number of years. The condition may be completely asymptomatic, present as non-specific lower back pain, or cause mild to severe pain, numbness or tingling in the posterior or lateral lower limbs and buttocks. Bladder function may also be impaired in severe cases.
Left untreated, a number of cases will improve, most will remain the same, and some will progress over time.
While the lumbar region is most commonly affected, do not forget cervical spinal stenosis, which can have similar features to lumbar spinal stenosis except that, in addition to lower limb signs and symptoms, patients may also have numbness, tingling, pain and manual dexterity problems in the upper limbs, and brisk reflexes.
Differential diagnosis includes vascular claudication and peripheral neuropathy. As mentioned previously, tumours, infection, fractures and disc herniation can also cause similar signs and symptoms.
The spinal canal dimensions are affected by position. In extension, the cross-sectional area is lessened, whereas in flexion the dimensions are increased. This explains why, in spinal stenosis, the leg symptoms are worse in the upright position but improve when leaning forwards, such as when pushing a supermarket trolley or riding a bicycle. These patients will also find it easier to walk uphill than downhill.
In comparison, patients with vascular claudication will experience constant leg pain with activities such as walking and riding a bicycle, irrespective of posture. Peripheral neuropathies are also common in this patient group, and are often secondary to diabetes or vitamin deficiencies. They tend to present in the classic glove-stocking distribution.
Other differentials such as tumours, infections and fractures present with pain that is constant, and may also disturb sleep. There is usually a history of trauma with fractures, while tumours and infections are generally accompanied by a feeling of malaise.
Diagnosis
Diagnosis is through clinical and radiological examination.
Clinical
Neurological examination is normal in most cases, but some patients can present with motor weakness, particularly of the L5 nerve root in the form of weakness of ankle dorsiflexion and big toe extension. Depending on the level of nerve root involvement, there can also be weakness of the hip flexors, hip abductors, the quadriceps, and knee flexors. If there are no findings on an initial exam, consider repeating the assessment after provocative stress tests, for example, by making the patient walk until the symptoms appear. Asymmetrical reflexes of the knee or ankle are consistent with spinal stenosis. Babinski or clonus signs should be negative in lumbar spinal stenosis. If they are positive, concurrent cervical spinal stenosis or other proximal cord or neurological conditions should be considered. The straight leg raise test is usually negative.
Remember also to check for signs of tumour, infection, fractures and vascular insufficiency.
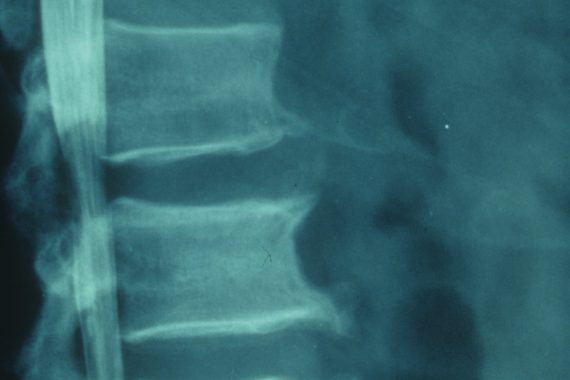
Radiological
MRI is the gold-standard for diagnosis, and is useful for surgical planning. It will also differentiate tumours, infections and acute fractures. Where there are contraindications to MRI, a CT scan with contrast (CT myelogram) can be used.
Management
Management is initially through non-surgical methods. Physiotherapy and a modification of activity, for example, using a walking aid, should be used, together with analgesia such as simple non-opioids like paracetamol and NSAIDs. If these methods fail, epidural steroidal injections can be tried. Light cardiovascular exercise can also help, with stationary cycling usually well tolerated because of the flexed position of the spine. Most patients are well managed through non-surgical methods and do not degenerate sufficiently to require surgery.
Surgery is considered once the symptoms are severely affecting the patient’s quality of life, the aim being to relieve symptoms in the lower limbs rather than the back. Patients with only lower back pain and no complicating conditions such as scoliosis are usually best managed non-surgically. The standard operation is decompressive laminectomy. Patients usually respond well to surgery, although complications are more likely as the patient gets older or if comorbidities are present.
Mr Colin Nnadi is a consultant spinal surgeon at Oxford University Hospitals NHS Foundation Trust
Jennifer Thorne is a medical student at the University of Malta
Resource
Garfin S, Herkowitz H, Mirkovic S. Spinal Stenosis. Instructional course lectures 2000;49:361-374









