Non-Covid clinical crises: Grossly abnormal LFTs
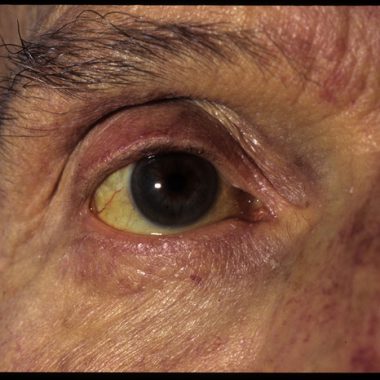
The key scenarios are jaundice and markedly deranged liver enzymes in the absence of jaundice. Jaundice will usually require investigation and the urgency and route depend on the level and associated symptoms. A bilirubin of <100 can be investigated in primary care unless there are symptoms of cholangitis.
An ultrasound scan is the key test and should ideally be done within a week. If the scan does not show biliary obstruction, look for obvious cause as per deranged liver enzymes. People are drinking more at this time of stress and confinement so think of alcohol. If jaundice is progressive then you will need to ask gastroenterology advice.
Most trusts have 2ww triage clinics and patients over 40 and with jaundice, should continue to go via this route; if the bilirubin is <100 you can do a community ultrasound first and act on the result. This will cover most patients at high risk and allow a risk-based approach to further tests. Those with biliary obstruction fall into the category of people who will need to brave Covid-19 and visit a hospital.
Deranged liver enzymes without jaundice are less urgent. If a patient presents classically with hepatitis with ALT in the hundreds to thousands check for new medicines (new in the last two months) and stop, think of CBD stones (ALT does go up in biliary obstruction) so if it is painful an ultrasound scan is again the best test.
If possible, send blood for Hep A, B, C and E serology plus liver autoantibodies and immunoglobulins. These tests will cover all potentially serious diagnoses.
You can ignore asymptomatic more minor elevations of liver enzymes until Covid-19 is over. Minor is defined as ALT<500. Weight loss and cholestatic LFTS (grossly raised GGT and ALP) can be liver metastases so an ultrasound again is needed but can be in primary care.
If ALT>500, suggest early repeat (within two weeks) and refer if rising or if jaundice develops (will need to do this via local agreed urgent route as this doesn’t fit 2ww). Any level of ALP/GGT can be put on hold if the ultrasound is normal.
Professor Stephen Ryder is consultant hepatologist at Nottingham University Hospitals NHS Trust and honorary professor, University of Nottingham, School of Medicine. Professor Ryder is also chair of the Hepatitis C Coalition.
Visit Pulse Reference for details on 140 symptoms, including easily searchable symptoms and categories, offering you a free platform to check symptoms and receive potential diagnoses during consultations.







