How to recognise amelanotic melanoma

Once in a lifetime: In the latest in our series, GP with specialist dermatology interest Dr Anjali Pathak discusses the rare but significant form of skin cancer termed amelanotic melanoma
What is it?
Amelanotic melanoma (AM) is a variant of melanoma in which malignant melanocytes produce little or no pigment. Lesions may appear pink, red or skin-coloured rather than dark brown or black. They can present as macules, plaques or nodules and may be smooth, scaly, ulcerated or crusted. While most cases occur on sun-exposed skin (as shown in image 1), amelanotic melanomas can also arise on acral sites such as palms, soles and nail beds, or on mucosal surfaces, making them even more difficult to recognise.

Image 1. Amelanotic melanoma on nose. Image author’s own: reproduced with permission
Without pigment, AMs rarely meet the ABCDE criteria (Asymmetry, Border irregularity, Colour variation, Diameter >6 mm, Evolving). They are therefore easily mistaken for benign or less aggressive lesions. This diagnostic difficulty contributes to later presentation and, on average, a greater Breslow thickness at excision. Amelanotic melanoma often presents as the nodular subtype, which is known for its aggressive vertical growth, a feature that makes nodular melanomas disproportionately amelanotic.
The risk factors for amelanotic melanoma are largely the same as for pigmented melanoma, and recognising them can help guide a GP’s index of suspicion. Patients with fair skin, blonde or red hair, blue or green eyes and a tendency to burn rather than tan are at heightened risk, as are those with a history of blistering sunburns in childhood. A family history of melanoma, the presence of multiple or atypical naevi and immunosuppression (for example following organ transplantation or long-term immunosuppressive therapy) also increase risk. Older age is another important factor, with amelanotic melanoma more commonly diagnosed in patients over 60. In primary care, awareness of these background risks can be useful when assessing ambiguous non-pigmented lesions and should further lower the threshold for urgent referral in primary care.
How rare is it?
Amelanotic melanomas are uncommon, accounting for 2-8% of all melanomas, though some studies report higher proportions if partially pigmented lesions are included. In the UK, melanoma overall is the fifth most common cancer, with around 17,500 new cases diagnosed every year (2017–2019). This equates to 48 cases every day and 5% of all new cancer diagnoses. Given that AM constitutes a small minority of these, many GPs may only ever encounter one or two confirmed cases during their career.
Early clues and red flags
The Glasgow 7-point checklist remains a useful tool for referral. While its major features such as change in size, shape, or colour are often less relevant for amelanotic melanoma, its minor features can be particularly important. A score of three or more should prompt referral, especially when features such as inflammation, oozing or bleeding, and change in sensation are present.
In practice, several additional clinical clues can help. A pragmatic way of remembering them is the ‘3 Rs’: a lesion that is red, raised and showing recent change. The ‘EFG’ rule is also valuable in nodular forms – where lesions are elevated, firm and growing steadily over three to four weeks. Any lesion that looks like the ‘ugly duckling’, meaning different from the patient’s other moles, deserves suspicion, as does one with a clear history of rapid evolution. Lesions that are friable, ulcerated or non-healing despite appropriate management should raise concern, as should nodules that feel unusually firm to the touch. Dermoscopy, if available, may also reveal atypical features such as polymorphous vascular patterns (as in image 2) or milky-red areas that are not visible to the naked eye.
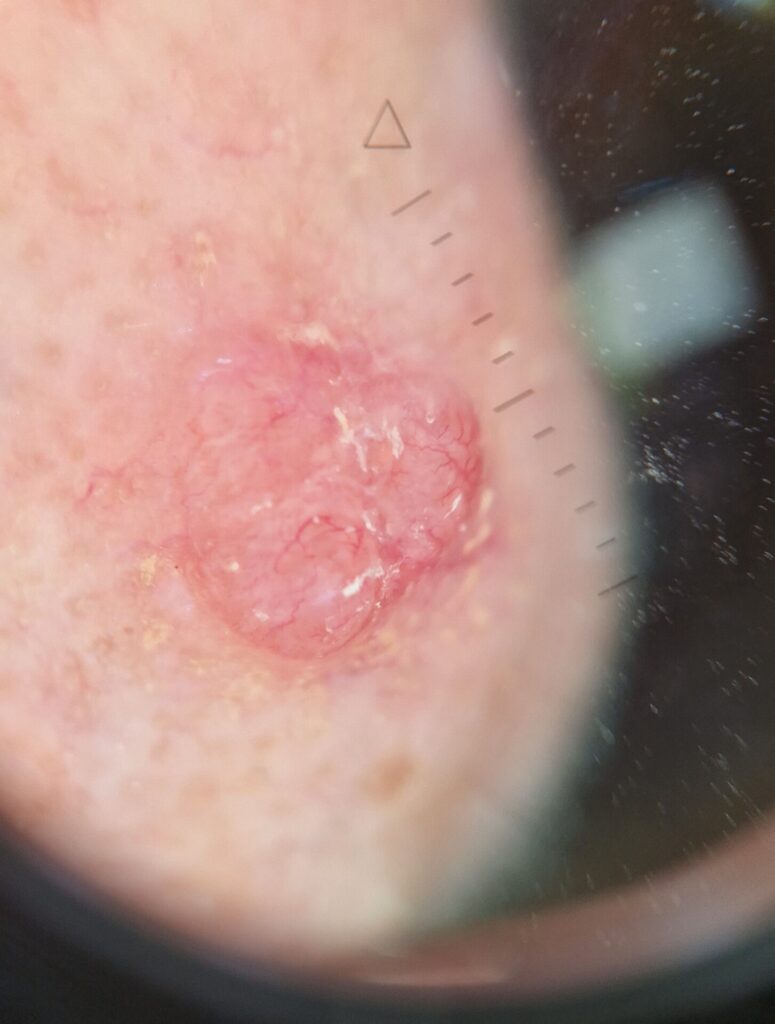
Image 2. Dermoscopy image of amelanotic melanoma showing polymorphous vascular pattern. Image author’s own: reproduced with permission
In line with NICE guidance on suspected cancer recognition and referral (NG12), any lesion raising suspicion should be referred under the urgent suspected cancer pathway. Although NG12 refers specifically to pigmented lesions, the same threshold should apply to non-pigmented but evolving, non-healing, or atypical lesions. In other words: if in doubt, refer.
May be confused with…
Amelanotic melanoma is often described as a ‘great masquerader’ because of its ability to mimic a wide range of common conditions.
Rapidly growing, ulcerated nodules may easily be mistaken for a pyogenic granuloma, while pink, pearly nodules or superficial scaly patches could suggest basal cell carcinoma.
Squamous cell carcinoma in situ (Bowen’s disease) can present as red, scaly patches, and keratoacanthoma often appears as a dome-shaped lesion with a keratinous plug, both of which can overlap with AM.
Other benign mimics include dermatofibroma, which typically forms a firm nodule that can sometimes be amelanotic, or Spitz naevus, particularly in children. Inflammatory skin conditions such as eczema, psoriasis or even warts may further complicate the picture.
In primary care, pitfalls include treating presumed infection with antibiotics, or assuming a lesion is a wart, skin tag or patch of eczema and prescribing topical steroids.
A ‘watch and wait’ approach can also lead to significant delay. Such missteps risk diagnosis only once the melanoma is thicker, when outcomes are poorer. Awareness of these traps helps ensure AM is considered in the differential earlier.
Usual treatment and prognosis
In secondary care, the cornerstone of management is wide local excision (WLE), with surgical margins guided by tumour thickness and discussed within the multidisciplinary team.
Sentinel lymph node biopsy (SLNB) is not recommended for stage IA melanoma, but may be considered in tumours ≥0.8 mm with ulceration or other high-risk features.
Prognosis is strongly linked to tumour thickness and ulceration. While early-stage melanoma has excellent outcomes, AMs are often diagnosed later, with thicker tumours and higher rates of nodal involvement. Registry studies consistently show that outcomes for amelanotic melanoma are worse than for pigmented melanoma, largely because of delayed diagnosis.
For advanced disease, treatment may involve systemic immunotherapy (anti-PD-1, anti-CTLA-4 agents) or targeted therapy (for example, BRAF/MEK inhibitors in mutation-positive patients), both of which have significantly improved survival in recent years.
Key points for GPs
Amelanotic melanoma is rare, but the absence of pigment should not reassure. Any new, evolving, firm, red, or friable lesion warrants urgent referral.
The key message is simple: not all melanomas are dark. Recognising this ‘once in a lifetime’ diagnosis in primary care could be lifesaving.
Dr Anjali Pathak is a GPwER in dermatology and visiting lecturer in clinical dermatology at the University of Hertfordshire
Sources and further reading
- Cancer Research UK. Skin cancer statistics (2017–2019)
- DermNet NZ. Amelanotic melanoma
- DermNet NZ. Dermoscopy of melanoma
- NICE. Suspected cancer: recognition and referral [NG12] Last updated 2025
- NICE. Melanoma: assessment and management. [NG14] Last updated 2022
- Sohail A, Kavaklieva S. Identifying the clinical and histopathological characteristics of amelanotic melanoma: a case series. Oxf Med Case Reports 2024;2024(4):omae029
Visit Pulse Reference for details on 140 symptoms, including easily searchable symptoms and categories, offering you a free platform to check symptoms and receive potential diagnoses during consultations.











