Meningitis B outbreak: what GPs need to know

GP Dr Toni Hazell outlines key information for GP practices about the current meningitis B outbreak, explaining how to deal with contacts and how this is funded, and how to manage queries and requests for vaccination from the wider public
The current meningitis B outbreak in Kent started on 9 March and, as of March 25, consists of 20 confirmed cases, three suspected cases and two deaths – latest figures here.
The outbreak is centred around a nightclub in Canterbury and is unusual because the peak of meningococcal disease is in infancy, with a smaller secondary peak in adolescents.1-3 It’s not completely surprising as living in communities such as military barracks or university halls of residence is known to be a risk factor for disease,3 and because the cohort currently at university have never been vaccinated against meningitis B.
GPs in Kent are at the epicentre of this, but practices all around the country may get calls from concerned parents, or from students home from Kent for Easter. There may also be requests for vaccination from those who aren’t eligible, as well as a lower threshold for people to present with symptoms which they think indicate meningitis.
What is the GP practice role in managing the public health response?
Contacts in the Canterbury area are being offered antibiotic prophylaxis and the meningitis B vaccine, dispensed from clinics set up for this purpose.
Eligible groups are given in the box below.
Who is being offered antibiotics and meningitis B vaccine?
Antibiotic prophylaxis and meningitis B vaccination is offered to the following groups:4,5
- Close contacts of those with confirmed or suspected meningococcal disease.
- Those who live on Canterbury campus and some staff working or living there.
- Students who attend other universities in Canterbury where there has been a case and who have been advised by UKHSA to have prophylaxis due to close contact with a case.
- Students in years 11, 12 and 13 who attend a school/college where there has been a confirmed or probable case.
- Anyone who visited or worked at Club Chemistry in Canterbury between 5 and 15 March.
Starting with the cohort described above, they should all have been dealt with locally. However, GP practices are asked to prescribe for and vaccinate contacts who returned home before receiving antibiotics or vaccine.
The prophylactic antibiotic is a single dose of ciprofloxacin – doses in the table below. Chemoprophylaxis clears nasal carriage of meningitis B, preventing onward transmission.
Table. Single dose of ciprofloxacin for antibiotic prophylaxis:6,7
Age Dose ≥ 12 500 mg 5 – 11 250 mg 1 – 4 125 mg < 1 30 mg/kg (max 125mg)
The provision of antibiotic prophylaxis is not contractually core general practice; if unsure how it will be funded, practice managers should check with their ICB. Arrangements vary – some areas have a memorandum of understanding whereby practices can invoice the ICB, and elsewhere it is commissioned from a specific site such as an out-of-hours centre. Expecting practices to absorb this work without resources is unacceptable and practices experiencing this should contact their LMC.
Vaccination is resourced via the usual item of service payment.
How should GPs assess and advise patient concerned they may have meningitis? When should meningitis be suspected and patients referred?
Patients other than the cohort above may approach their GP worried about symptoms; to advise, we need to understand the strains of meningitis, who they affect and how the disease presents – as well as NHS vaccine provision and the reasons behind vaccination decisions, which will be discussed in the following sections.
Neisseria meningitidis is a Gram-negative diplococcus found in 12 capsular groups – A, B, C, E, H, I, K, L, W, X, Y and Z. It is a common nasopharyngeal commensal, particularly in adolescents and young adults, and usually does not cause clinical disease.
Invasive meningococcal disease is most commonly caused by strains B, C, W and Y. We don’t understand why some people develop it and others don’t – risk factors include smoking and preceding viral infection, as well as the living conditions already mentioned.3
The commonest presentation is meningitis or septicaemia, but other clinical manifestations include pneumonia, myocarditis, endocarditis and pharyngitis.3
Key symptoms and signs of meningitis are given in the box below; clinical presentations should be managed in the normal way and the incubation period is 2-7 days.7 Some patients will get a mild prodromal illness before becoming more unwell, whereas others will progress from first symptoms to septicaemia and death within 24 hours.
Key symptoms and signs of meningitis
- High temperature.
- Headache
- Stiff neck.
- Dislike of bright lights.
- Cold hands and feet.
- Raised pulse or respiratory rate.
- Vomiting.
- Confusion or drowsiness.
- Muscle/joint pain.
- Skin which is pale, mottled, blotchy or has a petechial rash which does not fade under pressure.
- Seizures.
- In babies – refusal of feeds, general irritability, high-pitched cry, bulging fontanelle, being stiff or floppy and unresponsive.
If active invasive meningococcal infection is suspected then antibiotic should be given immediately, if stocks are readily available:7
- Benzylpenicillin IM: 2 g stat (for adults and children ≥ 10 years).
- Ceftriaxone IM: 2 g stat (for adults and children ≥ 9 years or ≥ 50kg).
The patient should be transferred immediately to hospital – if administering the antibiotic would cause a delay, it should not be given.
It’s important to stress that the UKHSA has advised that the risk of infection to the wider population remains low, even after this outbreak.
Invasive meningococcal disease is notifiable; doctors have a legal duty to notify public health at the point of suspicion – do not wait until a case is confirmed.5 Details of how to notify are here.
Should GP practices now be offering meningitis vaccinations to children or adolescents who did not previously take up the offer of their routine meningitis vaccinations?
The NHS meningitis vaccination schedule is given in the box below; the infant meningitis B programme began in September 2015,8 so only those who are currently up to the end of primary school age will have been entitled to it.
GP practices can give the catch-up meningitis B vaccine up to the age of 2, and catch-up meningitis ACWY vaccine up to the age of 25 (see box below).3,9 These are resourced under usual item of service payments, but GP practices cannot vaccinate outside of these parameters (except for those related to this outbreak as already mentioned).
NHS meningitis vaccines
- Meningitis B:
- 8 weeks, 12 weeks and 1 year.
- Catch-up available up to the day before the second birthday for those who have not received two doses.
- Meningitis ACWY:
- 14 years (given in school).
- Catch-up available up to the day before the 25th
If someone who has declined vaccination for other conditions as well as meningitis approaches the practice for a catch-up, it would be the perfect opportunity to suggest that they also consider MMR, given the current measles outbreak – this can be given at any age.10,11
The green book should be consulted for catch-up schedules for other vaccines – chapter 11 deals with immunisation schedules in general or the information can be found in the chapter dealing with that specific infection.11
How should we advise parents regarding children who missed out on the meningitis B vaccine because they were too old when it was introduced? Can they still access the vaccine – and is it worth having?
This group can’t currently be vaccinated on the NHS. The vaccine is available privately, but stock is currently difficult to come by, with many clinics and pharmacies holding waiting lists.12
Some charities have called for routine vaccination of adolescents against meningitis B.13 This was last discussed at a Joint Committee Vaccination and Immunisation (JCVI) meeting in June 2020, where it was noted that the incidence of invasive meningococcal disease in adolescents and young adults is not high enough for routine adolescent vaccination to be cost-effective.14 It was also noted that offering a booster in the teenage years to those who received the childhood vaccination does not significantly increase immunity. Also, while the available meningitis B vaccine protects the individual from disease it does not prevent carriage (and therefore transmission) of meningitis B.15
It is understandable that parents will be concerned at their inability to access an effective vaccine, particularly if their child is about to go on a school trip or another activity where they will be in close contact with many other children – to answer these questions it helps to understand the population incidence of meningitis B.
Meningococcal disease is much less common than in previous years – this trend is due to vaccination (which started in the UK in 1999 with the meningitis C vaccine) and can be seen in the graph below (Figure 1 from chapter 22, the green book).3,16
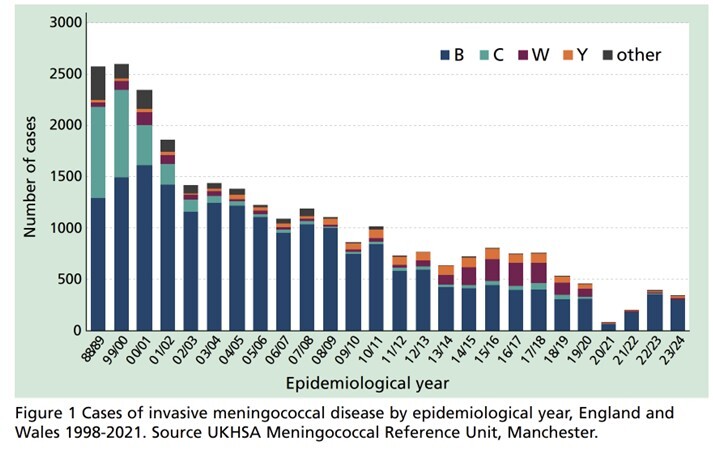
Source: UKHSA – green book chapter 22
There are around 300–400 cases of meningococcal disease in England every year –this is around half a case per 100,000 of the population, a statistic that could be made more real to a patient/parent by telling them this equates to filling Wembley stadium more than twice over to find one case of meningococcal disease. Schoolchildren under the age of 15 are at a relatively low risk (as seen in the graph below, figure 2 in chapter 22 of the green book). Parents can of course seek a private vaccine, but they may need to wait while stocks recover.
Source: UKHSA – green book chapter 22
Dr Toni Hazell is a GP in north London
References
- UKHSA. Cases of invasive meningococcal disease notified in Kent. March 2026.
- Surrey and Sussex LMCs. Reported outbreak of penicillin-resistant invasive Men B linked to the University of Kent. March 2026.
- UKHSA. Meningococcal: the green book, chapter 22. July 2025.
- UKHSA. Meningitis outbreak: what you need to know. March 2026.
- NHS Kent and Medway. Meningitis information hub. Who is eligible for preventative antibiotics and vaccines? March 2026
- UKHSA. Meningococcal disease: guidance on public health management. Last updated 2025
- NHS England. Outbreak of meningococcal disease linked to University of Kent and the area of Canterbury. Last updated 23 March 2026
- PHE. National childhood immunisation programme boosted by MenB vaccine. Aug 2015.
- NHS. NHS vaccinations and when to have them. Aug 2023
- UKHSA. Confirmed cases of measles in England by month, age, region and upper tier local authority: 2025. March 2026
- UKHSA. UK immunisation schedule: the green book, chapter 11. June 2025. https://www.gov.uk/government/publications/immunisation-schedule-the-green-book-chapter-11
- Boots. Meningitis B waiting list. As of 25.3.26. https://www.boots.com/information/meningitis-waiting-list
- Meningitis Now. No Plan B for Men B. https://www.meningitisnow.org/meningitis-now-stories/campaigns/no-plan-b-for-menb/
- JCVI. Minutes of the JCVI meningococcal sub-committee meeting. 20 June 2025
- UK Parliament. Meningitis: vaccination. Dec 2025
- Meningitis Now. Our history and achievements.
Visit Pulse Reference for details on 140 symptoms, including easily searchable symptoms and categories, offering you a free platform to check symptoms and receive potential diagnoses during consultations.









